Jogger’s Wenckebach
Report:
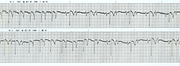
Sinus rhythm
Wenckebach (Möbitz 1) second degree AV block, atypical
Periods of 2:1 conduction (block)
Comment:
The patient may well have a mild form congenital heart block, but the progressive angina should call for evaluation of his coronary reserve. Angiography would be the best starting point at present. An exercise test should demonstrate improved conduction in uncomplicated congenital AV block and may, of course, indicate ischæmia.
In an ordinary jogger, “athlete’s heart” as the cause of AV block remains unlikely.
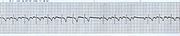
In both strips, the P waves are distorted by the overlying (?underlying) T waves. Below, in Fig 37a, (note a different lead, probably aVR), the three P waves before the first pause are almost completely disguised and one may think there are three junctional beats following a blocked P wave. That P wave is not blocked, but its (and subsequent) PR intervals are much longer than expected. Either a very atypical Wenckebach or an example of dual conduction. Confusingly, superimposition of P and T waves is called fusion in Wagner’s unfortunate rendering of Marriott’s famous book.27
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.