Runs of Anomalous Conduction

Report :
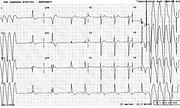
WPW syndrome
Atrial fibrillation
Runs of anomalous conduction (Wolff-Parkinson-White type ‘A’)
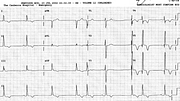
Borderline small voltage and T wave changes in frontal leads
Comment :
Syndrome, rather than mere conduction, because of the arrhythmia.
The patient is on sotalol and the ventricular rate is not as fast as usually seen in WPW atrial fibrillation. The anomalous complexes are too irregular for runs of VT ; some terminate quite long cycles at the beginning and the end of the recording. As usual in WPW, the conduction is mostly anomalous, with one or two completely normal QRSs separating the anomalous runs.
This is somewhat arbitrary, but the QRS looks more above than below the isoelectric line in V1 – hence the designation as type ‘A’. It is easy to remember left (‘A’) and right (‘B’) bypass using V1 : ‘A’ for above, ‘B’ for below, as defined by Rosenbaum in the year I was born, 1945102. This original division has been refined since; the important thing here is the clear-cut Rs morphology in lead V2, confirming the left-sided bypass in this case103.
This patient was admitted to CCU for elective cardioversion ; this was abandoned after no less than four unsuccessful attempts and he was sent home on increased dose of sotalol (60 mg BD) and enoxiparin. This blocked the Kent bundle quite well (116a).
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.