AV Dissociation in VT
Report:
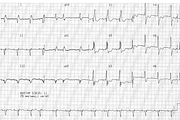
Sinus tachycardia 127/min
Left atrial abnormality (LAA)
First degree AV block (PR 0.22”)
Axis -100o (Northwest, no-man’s land, “nonsense” axis)
Probable left anterior hemiblock
Right bundle branch block
VEB, probably fusion beat (5th in V1)
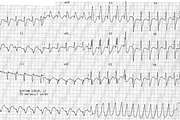
Ventricular tachycardia 175/min (rhythm strip)
Fusion beat (first VT complex)
AV dissociation
Comment:
The P waves can be seen to march through the VT at the same rate as before the paroxysm. Of the 10 P waves involved, 7 can be clearly discerned as “bumps” occurring in the expected places. The remaining three are completely hidden by the broad R waves of the VT.
AV dissociation is, on statistical grounds, evidence for the ventricular (rather than aberrant supraventricular) origin of the broad complex tachycardia129. This evidence is not absolute: “You cannot tell a pacemaker by the company she does not keep!”4
Below (Fig 174a) is the 12-lead ECG obtained after the tachycardia. Its arm leads are reversed, perhaps due to the excitement generated by the occasion.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.