Slow Bidirectional Tachycardia
Report:
Bidirectional tachycardia 104/min
Retrograde VA conduction
Junctional escape beats
AV dissociation
Sinus rhythm 95 – 98/min
Overdrive (post-ectopic) SA suppression
Comment:
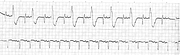
The rhythm is obviously bigeminal, with narrow rSR’ complexes followed by plump R complexes; both leave retrograde P waves in their wake. It is tempting to postulate reentry involving those retrograde P waves, but the cycle-length sequence and the QRS morphology does not support it. Any reentry present would be taking place down in the ventricles, involving the two bigeminal QRS complexes. These complexes both resemble – however remotely – RBBB; both are clearly different from the sinus rS complexes. If frontal leads were available, the bigeminal complexes would be likely to show alternating right and left axis deviation typical of bidirectional ventricular tachycardia. Its reentry has been shown to involve the two fascicles of the left bundle branch141. The strips show its typical appearance in V1 – except that most cases are faster.
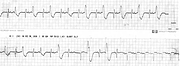
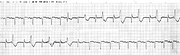
At the end of the top strip, bigeminy ceases and a junctional escape complex appears (the last in the top strip); a dissociated sinus P wave may be contained in it. The next escape beat has a more definite sinus P wave at its onset. Sinus rhythm takes over from then on, showing the rSR’ beats for what they really were: fascicular ventricular ectopics. (They come after longer cycles, during bigeminy, than ordinary sinus beats during sinus rhythm – there is no reason for them to be RSR’-aberrant.) The lower strips show another run of bidirectional tachycardia, this time with both its onset and termination.
Most cases of this rare rhythm are due to digoxin toxicity. This one is an exception.
Another episode is shown in Fig 205b.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.