VT or SVT in a Patient with Known LBBB?

Report:
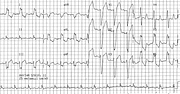
Ventricular tachycardia 174/min.
Comment:
The QR morphology in lead V1, however, is that of VT, unless there was a previous anteroseptal infarction. The marked LAD -90o is neither here or there, diagnostically. Interestingly, a recent study using the Brugada algorithm in a Californian Casualty (Emergency Room) found disagreement between the physicians 22% of the time143!
The decisive factor is the presence of LBBB in sinus rhythm: aberration preserves the original conduction defect2, or adds to it.
There are, admittedly, cases of identical QRS morphology in VT (or VEBs) and sinus rhythm144, but this is obviously not the case here.
This VT should logically originate from the left posterior fascicle of the blocked left bundle branch.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.