Alternate Cycle Antecedent P Waves


Report:
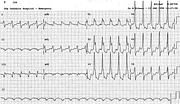
Ventricular tachycardia 125/min
Probable 2:1 retrograde conduction
Comment:
The diagnosis of VT is supported by the QRS duration of 0.18”, the indeterminate abnormal axis and the left rabbit ear in V1 being taller than the right. The relatively slow rate is very likely due to previous sotalol therapy. A dissociated sinus rhythm ECG is shown below (Fig 21a).
This was a rather confusing ECG in that the two sharp P waves in V1 look like sinus P waves. In the L2 rhythm strip, the predominantly positive “bumps” can also pass for sinus P waves, although the real sinus P waves are different (Fig 21a below).
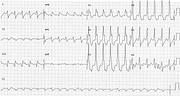
Other VT tracings are more informative. The first one, taken hour and a half later (Fig 21a), has rather regular positive atrial waves (?sinus) at about 80/min; these appear dissociated from the 140/min VT. The bottom one Fig 21b), 146/min, taken 5½ hours later, shows regularly recurring obviously retrograde (negative in L2) P waves, probably in retrograde Wenckebach conduction. Looking back at the index trace, the P waves are not only smaller and narrower than sinus P waves, but appear biphasic in both L2 and, especially, aVR. Both upright24 and biphasic25 retrograde P waves have been reported. The marked (0.40”) retrograde block in the (2:1) conducted ones in the index trace can be accounted for by sotalol and verapamil therapy.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.