Bigeminal Ventricular Tachycardia


Report:
Ventricular tachycardia 173/min
Alternating cycle length
Comment:
The patient had presyncopal paroxysms of VT, though to be SVT by many because of its relatively narrow QRS. They were even more convinced when, in Casualty, he reverted to sinus rhythm with two doses of 2.5mg verapamil IV. He was fortunate: this is a fascicular26, verapamil-sensitive variety of VT27; otherwise, verapamil would have probably disagreed with him in a major way28.
There is a slow S downslope in V1, characteristic of ventricular ectopic origin. As to the alternans, a purist would have trouble diagnosing it: the cycle lengths are varying, mostly alternating themselves. This can of course alter ventricular conduction.
Alternate cycles also have a sharp deflection in their waves, consistent with retrograde conduction; in the first half of the trace, it appears to be 2:1. The presence of retrograde 2:1 block is in itself evidence of ventricular ectopic origin of the tachycardia5. It is rarely mentioned because it is rarely seen.
His sinus rhythm trace, with a single VEB like those of the VT, is shown in Fig 22a. The VEB itself is an R-on-P phenomenon, showing an intellectually reassuring (for diagnosis of VT) A-V dissociation.
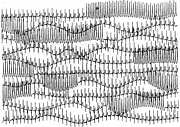
A Holter monitor sheet with frequent VT runs is shown in 22b. Voltage alternans is clearly visible in the top strip.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.