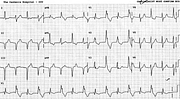
Bidirectional AIVR
Report:
Alternating (bidirectional in some leads) accelerated idioventricular rhythm
Comment:
At first glance, the trace suggests RBBB and ventricular bigeminy. It is quite regular and no definite atrial activity can be discerned, except for the wrinkle after the QRS in lead 3. It could be junctional (or main-stem) rhythm with VEBs in bigeminy, but the regularity of the ventricular cycles is somewhat against it: there are no premature beats.
At a faster rate, this could pass for an atypical form of bidirectional VT. The latter is, according to some theories, only half ventricular in origin. Most of those have alternating cycle length as well, anyway.
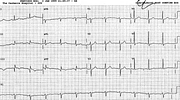
The QS complexes in the inferior leads may suggest inferior infarction, which the patient in fact had (below, Fig 220a), later to become inferolateral infarction.
In this setting (of reperfusion and inferior MI) the most likely diagnosis is AIVR, bidirectional from two foci or two conducting pathways . An idiofocal phenomenon (pace Schamroth). Does it matter? It does: idiofocal rhythms are tolerated, while bigeminal (or even frequent) VEBs would still, in most units, be treated in the wake of acute infarction.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.