Multiform Ventricular Tachycardia

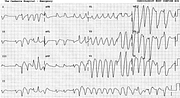
Report:
Atrial fibrillation
Runs of multiform ventricular tachycardia 150 – 180/min
Right axis deviation +165o
Probable right bundle branch block
Acute inferior infarction
Comment:
There are only four pure supraventricular beats to be seen – two before and two after the short VT run at the beginning of the recording. They look bizarre enough in their own right, with deep broad S waves in leads 1 and aVL and ST segment shifts rounded into the ensuing T waves: they would suggest ventricular ectopic origin were it not for their even more bizarre and faster neighbours.
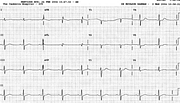
The next trace (Fig 226a), 15 minutes later, has only four VEBs and the diagnosis of RBBB can be made more securely. There are massive reciprocal changes in the chest leads, implying a large infarction; the RBBB itself suggests RV involvement.
The patient had a large obtuse marginal branch of the LCX stented, with surprisingly good ECG result on the tracing obtained 6 hours later in ICU. He had VF during the procedure and was intubated and ventilated for 24 hours – probably the best strategy for most arrests.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.