SVT with Right Bundle Branch Block Aberrancy
Report:
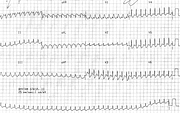
SVT 212/min.
Right bundle branch block (RBBB).
Right axis deviation +120o probably left posterior hemiblock (LPHB).
Comment:
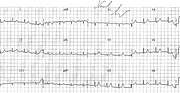
The likelihood of aberrancy rests with the rSR’ morphology in lead V1 and the absence of any bizarre features. Verapamil was used legitimately in this context; adenosine would have been even better, but was not yet available. She rapidly reverted to sinus rhythm (Fig 35a).
A verapamil-sensitive fascicular VT cannot be completely excluded. The rate is very rapid, but this, too, does not help distinguish VT from SVT, as readers of this Volume know or are about to find out. For a fast SVT, it is noteworthy that there is no electrical alternans. This may mean that there is no bypass tract, concealed or otherwise – the (micro)reentry is a nodal one.
Retrograde P waves are seen in most leads; they do not advance the diagnosis.
The sinus rhythm ECG is normal apart from small voltage and borderline ST/T changes. The reason for the former was not clinically obvious; the latter were uninterpretable in view of the preceding SVT.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.