VT Cardioversion: From Bad to Worse

Report:
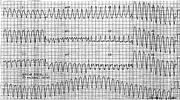
Broad complex (QRS 0.14”) tachycardia 204/min
Ventricular fibrillation (post 150 Joule DCC)
Sinus bradycardia (post 300 Joule DCC)
Normal sinus rhythm
Comment:
The synchronised countershock fell on the terminal QRS complex, well away from the succeeding T wave (just before the arrow, second strip, where the trace disappears).
It is by now old wisdom that, while there are many patients who cannot be helped, there are none that cannot be harmed! The decision to apply DCC to a symptomatic VT was a reasonable one, but one cannot help being a little shaken when VF appears instead of sinus rhythm! Luckily all ended well.
The 12-lead ECG (Fig 37a) is more convincing of VT than the rhythm strip taken from the vicinity of V2. It has monophasic R waves in V1 and deep QS in V3-6, with classical Northwest axis.
Xylocaine is an excellent, very safe drug; it is a pity that it is not a little stronger.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.