Arrhythmogenic Right Ventricular Dysplasia


Report:
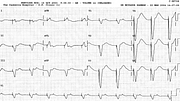
Ventricular tachycardia 162/min
Comment:
The patient had dilated right atrium and ventricle, with normal, mildly hypertrophied left ventricle. The coronary arteries were also normal. In Casualty, adenosine 6 + 12 mg, verapamil 2.5 mg, then sotalol, 60 mg were used; the VT became “pulseless” and DC countershock was required in a hurry.
This is a right ventricular VT in that it has a basic LBBB configuration, provided there is no coronary artery disease37. The tachycardia is easily distinguishable from LBBB aberrancy due to the slow S wave descent in lead V1. The left axis deviation is of no diagnostic value against aberrancy, but tends to differentiate ARVD VT from the RV outflow tract VT: the axis in the latter is right or normal. Left axis deviation is common in ARVD VT38.
Post-cardioversion ECG (Fig 39a) shows 1o AV block, LAHB and non-specific ST/T changes. The single VEB present is of the same morphology as the VT; it has a fully compensatory pause. This may be used to diagnose the VT, retrospectively. Nothing in the trace, however, is particularly suggestive of ARVD: no epsilon waves, no prolongation of V1 complex compared to V6, no anteroseptal T wave inversion.. Insofar as I know, this patient has only one major (selective RV cardiomyopathy) and one minor (VT of appropriate morphology) criterion for ARVD39.
The patient was later paced for AVB induced by anti-arrhythmic drugs (Fig 39b).
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.