Sotalol Torsades de Pointes


Report:
Sinus rhythm 67/min
Borderline first degree AV block
PR 0.20”
VEBs, frequent
Runs (3-beat, 5-beat) of multiform ventricular tachycardia
Incomplete LBBB
Prolonged QT interval
Comment:
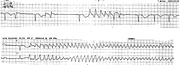
The patient’s torsades (Fig 56a) were treated by MgSO4, then xylocaine, then DC countershock in CCU. Sotalol has now replaced flecainide as leading cause of iatrogenous torsades in this hospital. Drug-induced (acquired) long QT syndrome has been reviewed recently54.
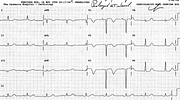
The important distinction between torsade de pointes and multiform VT rests on underlying bradycardia and prolonged QT interval being associated with the former. In sustained tachycardia, the observation of “spindles” and axis rotation does not distinguish between the two. A representative 12-lead ECG in sinus rhythm is shown below (Fig 56b).
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.