Ventricular Tachycardia: RV1

Report:
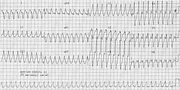
Ventricular tachycardia 220/min.
Comment:
The patient's age and the relatively fast rate must have influenced the first choice of aberrancy in the Casualty report. The "VT with underlying WPW", however, suggests diagnostic skills beyond electrocardiography!
The tachycardia itself has monophasic R wave in V1 - unlikely to represent RBBB aberrancy and a marked RAD not morphologically suggestive of LPHB aberrancy (where a qR in inferior leads would be expected). Combined RBBB/LPHB aberrancy is relatively uncommon78.
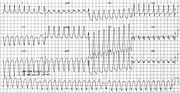
The sinus rhythm ECG is shown below (Fig 80a). It's sole abnormality is T3 > T1 , possibly a transient aftermath of the tachycardia itself. A VT recurrence in the CCU, this time also with RV1 but LAD and probable fusion beats, is shown on the following page (Fig 80b), where QS in V6 puts paid to any notion of WPW conduction.
Verapamil therapy of possible VT represents a physiological and medico-legal challenge best avoided79 On the other hand, verapamil-sensitive VT is a distinct, however heterogeneous, entity80.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.