Monomorphic Ventricular Tachycardia: Minuscule V1 Rabbit Ears


Report:
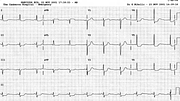
Monomorphic ventricular tachycardia 188/min
Comment:
The monophasic R complex in V1 has two small “rabbit ears”; the left one is mostly taller than the right (looking at the rabbit from behind). This is a classic marker of ventricular ectopic origin10. In this example it is barely perceptible and even less so in the VT recurrence a year later (Fig 9b). If the right one is taller, the probability of ectopy is only 50% - one may as well toss a coin. Of course, a monophasic R or a qR in lead V1 indicates ventricular ectopy in its own right. The LAD in the frontal plane remains non-contributory.
There was no response to Xylocaine in Casualty and the VT was cardioverted by a 200 Joule countershock. Xylocaine is relatively non-toxic and one cannot argue too much against its use as a first-line therapy of VT. On the other hand, it is not the most potent of antiarrhythmics. Procainamide or amiodarone appear better; perhaps our manuals should be re-written11.
Post-cardioversion ECG (Fig 9a), like in a previous case (Case 8) showed marked ST segment depression, indicating an underlying coronary artery disease. Perhaps immediate post-tachycardia traces are not the best ones to base one’s diagnosis upon: this patient had normal coronary arteries at angiography.
A good example of rabbit ears is seen in the following case (Fig 10).
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.