AV Block with Low Output
Report:
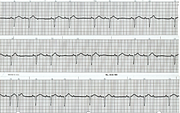
Sinus tachycardia
Second degree AV block, Möbitz 1 (Wenckebach)[!xe "AV block:second degree:Möbitz 1" \b!]
2:1 & 3:2 conduction
Comment:
Low output a fortnight after the acute event is difficult problem. The best strategy is to try and ‘stick it out’ provided no obviously reversible component of the low-output state can be identified and treated. The AV block in this setting may have been contributing to the problem and the obvious solution would be to institute sequential A-V pacing. Simply, increase the heart rate, if the remaining coronary system will wear it.
Another approach would be to start aortic counterpulsation and perhaps perform a catheter study if reversible ischæmia could be demonstrated by radionuclide imaging.
Atropine is usually not useful at this stage (long after the acute infarction), but aminophylline has been used more successfully.
The block resolved over the ensuing four days without any additional therapy and the patient improved; dobutamine was replaced by hydrallazine. Dobutamine infusion over several days is a recognised therapy for cardiac failure43; its benefits often outlast the actual infusion. Milrinone or levosimendan can be tried instead. For those who are difficult to wean off dobutamine, hydrallazine may be a useful step-down drug44.
Electrocardiographically, the strips are a typical 2:1 AV block that reveals its nature by slipping into 3:2 Wenckebach (bottom strip). Dig the break, Marriott would say. In the first Wenckebach sequence, the blocked P wave is invisible, masked by the QRS complex. In the second sequence it is partly visible between the end of the QRS and the onset of the ST segment. The conduction times are prolonged throughout.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.