ST Elevation or Non-Q Infarction?

Report:
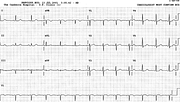
Sinus rhythm 87/min
ST/T changes c/w infarction/ischæmia
Comment:
This type of tracing is difficult to define. ST segment elevation infarction requires, by definition10, 1 mm elevation in at least two contiguous leads sustained over 30 minutes. Here the elevation in confined to V1 (aVR not counting), with no known time frame and (possibly reciprocal) ST depression in multiple leads. Or, aVR counting, the contiguity is only a paper, rather than electrical, contiguity. The overall appearances are similar to main left coronary artery stenosis in presentations of acute ischæmia; this patient, with history of remote CABGs for triple vessel disease, may well have had a “main left” equivalent.
The ECG became almost normal over 5 hours (Fig 12a), but the cardiac injury markers were quite elevated: an infarction had occurred. The VEBs in V1 knew it11 (Fig 12b). In fact, lead V1 in the original trace also knew it: its ST elevation, shared by the neighbouring leads or not, certainly “looks” infarctional: it has that upward bulge into the T wave. Like pornography – one knows it when one sees it, but it eludes definition.
The foregoing supports the term non-Q infarction as the best descriptor of what actually happened. But we know what happened only through high troponin and CPK values: the acute episode could equally have been ischæmia rather than infarction.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.