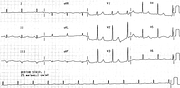
WPW ‘A’ Mime of Inferoposterior Infarction
Report:
Sinus rhythm 68/min
Wolff-Parkinson-White type ‘A’ conduction
Comment:
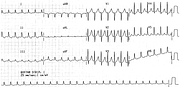
The QRS appears narrow and the PR interval normal in several – in fact, most – leads. On the other hand, the latter is completely effaced by a δ wave in V2 and V3. There is concordant positive precordial pattern. Best of all, there is a narrow-complex SVT 150/min preceding this trace (Fig 18a), but one is not to know that from the previous page! That may well have been the cause of his chest “tightness”.
The original SVT was much faster, but slowed down to 150/min with sotalol. The drug may have exerted a balanced slowing of both the normal and the accessory pathway, preserving the reentry. By then the patient’s medical records were brought up (revealing WPW syndrome) and procainamide given in view of its known blocking properties of the bundle of Kent. It worked, but it was overegging the pudding a little: any ordinary AV nodal blocker available in 1994 (e.g., verapamil) would have interrupted the SVT. Even digoxin.
Sotalol, like flecainide or procainamide is better used for AF in WPW if immediate defibrillation is not necessary.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.