Right Ventricular Infarction or Prinzmetal Angina?
Report:
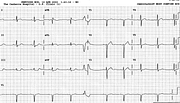
Sinus rhythm 78/min
SVEBs, one aberrant, two blocked
Wenckebach phenomenon
Acute inferior infarction
Right ventricular infarction
Left ventricular hypertrophy with ST/T changes
Comment:
The diagnosis of Prinzmetal angina was suggested when serial CPK levels remained within normal limits and the ECGs failed to evolve any Q waves. Echocardiogram showed dilated RV and RA, and suggested pulmonary hypertension with normal LV systolic function. On its face value, the ECG shown would have to be reported as infarction. The presence of pulmonary fibrosis and hypertension may account for the dilated right-sided chambers, but may also predisposed to their infarction or ischaemia. As Oscar Wilde puts it26, the truth is rarely pure and never simple!
The pauses, the setting of inferior infarction (or ischæmia) and the observed variation in the PR intervals all suggest Wenckebach second degree AV block as the mechanism. This is not so: both pauses are in fact due to Marriott’s commonest causes of pauses - blocked atrial ectopics.
The first pause is preceded by an aberrant SVEB with quite long – about 0.26” – P’-R interval. The blocked SVEB on top of the aberrant beat’s T wave may therefore be a reentry (echo) beat, engendered by the long P’-R interval. The aberrancy is of LBBB type – clearly supraventricular, with sharp S descent in V1 – and shares a rightward axis with the narrow-QRS beats. Rightward, but not quite right: RAD has not so far been described in LBBB aberrancy27.
Finally, is there LVH with ST/T changes or merely LVH voltage with reciprocal ST segment depression? Why should there be LVH in the first place? Unanswerable questions, except by vague generalities. ECG reporters should steer clear of those.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.