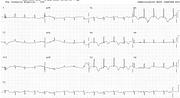
Massive ST Segment Elevation in Coronary Spasm




Report:
Sinus rhythm 93/min
Extensive acute anterior infarction
Comment:
The elevation settled rapidly and subsequent angiography documented normal coronary arteries. The most likely explanation is spasm, which may have caused near-drowning in the first place.
The ECG appearance, however, is that of “tombstones” from acute infarction. In some large anterior infarcts lead 2 shows ST elevation as well. After all, lead 2 is the sum of 1 and 3; large ST elevation in 1 will “pull” the segment up if depression in 3 is smaller.
Spasm is of course indistinguishable from thrombotic events electrocardiographically. In Figs 51c and 51d below, the appearances are similar to those in the preceding case, but the cause was a fixed proximal LAD obstruction in a 44 year old man. All the inferior leads show more conventional reciprocal ST segment depression.
A trace 5 hours later, with the patient ventilated in ICU for cardiogenic shock persisting after angiography, is shown on the back. Troponin levels rose to over 180 µ/L. He recovered but was left with marked LV dysfunction.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.