Wrong Reason for the Right Report
Report:
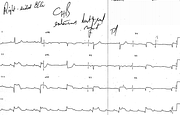
Sinus tachycardia 128/min
Third degree AV block
Junctional escape rhythm 38/min
Acute inferior and right ventricular infarction
(Right-sided V leads as labelled)
Atrial infarction
Comment:
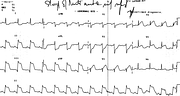
The report followed a previous one, on a preceding ECG taken on the same day which indeed showed both inferior and anterior infarction (Fig 73a). It is understandable, psychologically, to have diagnosed “extensive anterior infarct” on the appearance of also infarctional right-sided chest leads. Or, repetition compulsion?
The patient was in cardiogenic shock from the extent of his infarction and the presence of right ventricular infarction and complete AV block. Atrial infarction (seen as PT segment elevation in 2 and aVF) did not help, either, but in view of the CHB its impact on the atrial transport would be of little moment.
In the tracing below (Fig 73a), the reciprocal ST segment depression in both 1 and aVL suggests the RCA as the culprit vessel. Depression in V1-2 means that the elevation in the remaining precordial leads is not – as it sometimes may be53 - an expression of right ventricular, rather than a separate anterior, infarction. It is likely that the acutely occluded RCA had been supplying distal LAD artery via collaterals.
The patient survived extensive support and interventions and did surprisingly well.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.