Inferior MI, VEBs & Persistent Wenckebach

Report:
Sinus tachycardia 104/min
VEBs, frequent, multiform
Second degree AV block, Möbitz 1 (Wenckebach)
Late transition
Nonspecific intraventricular conduction delay (IVCD)
Acute inferior infarction
Anterolateral ST/T changes c/w MI/ischæmia
Comment:
The anterolateral ST/T changes are new and likely part of the inferior infarction; their location makes them unlikely to be reciprocal or to represent “independent” ischæmia. They are reported separately purely for descriptive purposes. The anteroseptal ST depression, however, is reciprocal and is not reported. In the presence of an obvious infarction it is best not to read too much into the ST/T changes elsewhere.
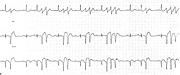
There are two consecutively conducted P waves, before 5th and 6th complexes, showing an increase in the PR interval, signifying Wenckebach conduction. There and elsewhere, full Wenckebach cycles take place, all terminated as expected by blocked P waves. What is not expected is that the frequent VEBs do not interfere with the sequences. This is most likely due to a two-level block61.
Yet another block is present here: the IVCD. Once upon a time it would have been called periinfarctional block. The term has no specificity and is best forgotten.
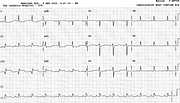
Her ECG three hours later is shown below (Fig 86a). A rhythm strip showing alternate-beat Wenckebach is shown in Fig 86b.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.