Ostium Primum ASD
Report:
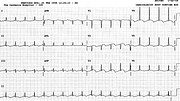
Sinus tachycardia 137/min (up to 133/min normal for below 4 years)
Left axis deviation –60o
Possible RVH (5mm R wave in V1 after 6 months of age)
Comment:
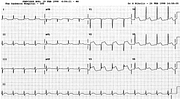
The rR’ in V1 is consistent with but not diagnostic of RVH: it can always be an RSR’ with slightly displaced electrode. Over 90% of ASDs (primum or secundum) have an RSR’ pattern in V1, perhaps though the hypertrophy of crista supraventricularis. A pure R wave would be better, and a qR or QR best of all. Oddly enough, such qR appeared after draining 400 cc pericardial effusion (below), along with a general increase in voltage. Lead V3 is missing because of the dressings.
The LAD is morphologically indistinguishable from LAHB. It is most commonly seen with endocardial cushion defects in children; ostium primum ASD is the commonest one seen in our hospital.
Of all the congenital cardiac repairs, that of an ASD is most likely to cause postoperative pericardial effusion or tamponade73.
It does not always happen, but considerable voltage drain followed the drainage (Fig 103a). I can only speculate this is because her pericardium was normal, unlike that of patients with inflammation or tumours.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.