Right Atrial Abnormality

Report:
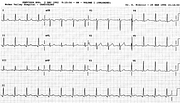
Sinus tachycardia 130/min
Right atrial abnormality
5 mm P wave in Lead 2
P wave axis + 90o
Vertical heart position
Comment:
The inferior ST segment depression (using T-P baseline) may be due, at least in part, to prominent Ta waves, inferred from 5 mm tall P waves.
The QRS complex is characteristically narrow in emphysema.
P wave axis seldom exceeds +90o; RAA is a rare cause of negative P in Lead 1. This patient’s P wave is invisible in Lead 1, completely isoelectric; the axis is therefore +90o.
Below (Fig 135a) is another cor pulmonale, in a 42 year old woman with fibrosing alveolitis. Her P wave in V1 shows prominent P-terminal force, but in V2 it is entirely positive and by V3 2 mm tall and pointed. This indicates, in the context, increased PTF due to right atrial enlargement.
Precordial T wave inversion is also in keeping with RVH. ST segment elevation in V1 can also occur in RV "strain", presumably present here with fibrosing alveolitis complicated by pulmonary infection.
The qR or qRs pattern in V1 is, in the absence of previous septal infarction, quite specific (but insensitive) marker of RVH or, more specifically, right atrial enlargement.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.