Pulmonic Stenosis


Report:
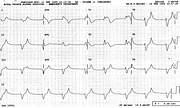
Sinus rhythm
Right axis deviation +140o
Right bundle branch block
Probable right ventricular hypertrophy
Comment:
The congenital PS was repaired 21 years previously; a late sequel was a right ventricular aneurysm, scheduled for elective repair later in the year.
The RVH could be inferred from the large-amplitude QR RBBB morphology in V1 and the marked RAD. The P waves are not helpful; there is, in fact, a soupçon of P-mitrale in Lead 1. Both surgery and RBBB (itself often resulting from surgery) can modify the ECG to the extent that conduction problems mask the underlying chamber hypertrophy. The sometimes used criterion of R wave in V1 > 15 mm has been rightly criticised by Schamroth104.
The Q wave is unusually deep and broad in V1 and the subsequent R wave is 0.12” long. A qR complex of normal duration is very specific for RVH in both children and adults; here one has to admit to some uncertainty.
In pulmonary stenosis the precordial T wave inversion goes much further to the left than in, say, tetralogy of Fallot.
Below (Fig 146a) is another RVH, with much smaller voltages, from a 60 year old lady with primary pulmonary hypertension. The intraventricular conduction is normal and the diagnosis clear-cut: RAD, RAA (in V2), qR in V1.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.