Right Ventricular Hypertrophy: Scleroderma
Report:
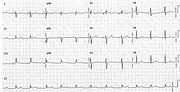
Sinus rhythm
Probable RAA
Right axis deviation + 130o
qRV1
Right ventricular hypertrophy
Comment:
The qR morphology of V1 is, by itself, evidence for right atrial enlargement as well as RVH; the prominent monophasic P in V2 supports it and increased PTF in V1 is consistent with it, too. There may also be some LAA (the commonest cause of increased PTF) but this patient has no reason for it clinically. She most likely has clinically silent pulmonary hypertension secondary to the connective tissue disease. Scleroderma cardiac disease is often secondary to renal or pulmonary involvement, but myocardial lesions are not exactly rare116.
The RAD is, electrocardiographically, very strong evidence for RVH; it helps differentiate RVH from anteroseptal infarction117.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.