It’s a Boy: Duchenne Muscular Dystrophy
Report:
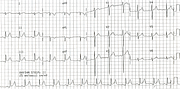
Sinus tachycardia 144/min
Axis +90o
Rs in V1 consistent with Erb-Duchenne (pseudohypertrophic) muscular dystrophy[!xe "Duchenne (pseudohypertrophic) muscular dystrophy" \b \i!]
Comment:
The characteristic feature of Duchenne dystrophy is the dominant R wave in lead V1. It has been related to fibrosis and hypertrophy of the posterobasal portion of the left ventricle. Tall right precordial R waves are often associated with Q waves in limb or left precordial leads; the Q waves seen here are, however, within normal limits. The ECG presentation of Duchenne dystrophy is thus indistinguishable from posterolateral myocardial infarction128.
Not all the patients with Duchenne dystrophy develop the characteristic ECG pattern. Below (172a) is an example from a 15 year old dying from respiratory muscle involvement. Early transition with prominent R in V2 is suggestive, but far from typical of anything in particular.
Yet another example is shown in Fig 172b, about to die in four days at the age of 21, with LAD -45o, presumably fibrosis involving the anterior superior division of the left bundle branch. The appearance is the same as any LAHB, except for much smaller than usual voltages.
Fig 172c exhausts my collection. It’s an 11 year old with fairly typical tracing, suspected by the reporting Cardiologist of having inferior infarction or hypertrophic cardiomyopathy, with advice the patient needs investigating. Not this one.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.