Sluggish Performance of Fat Complexes
Report:
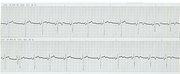
Atrial fibrillation with controlled response (top & bottom)
Mean BP 85 & 83 mmHg
Pacemaker rhythm (middle)
Mean BP 68 mmHg
Comment:
The slight asynchrony in contraction secondary to LBBB-type conduction becomes significant in a critically impaired ventricle165. Non-ischaemic chest pain may also result166.
This is not due to abolition of atrial transport by ventricular pacing: the patient is already in AF.
More of the same is illustrated below (Figs 236a, 236b). Ideally, the patient should have developed LBBB of his own; then the ventricular pacing should make no difference! A bad taste joke one says on the rounds.
Tall T Waves: Myocardial Rupture
Report:
Sinus rhythm
Third degree AV block
Junctional escape rhythm 43/min
Prominent T waves
Comment:
A rare cause of tall T waves, not unlikely in this case, is free wall rupture167. Other causes (infarction, reciprocal change to remote infarction, hyperkalæmia) cannot be excluded; however, sudden EMD remains, to use D. H. Spodick’s tongue-in-cheek term, ‘suggestoid’ of rupture. He actually refers to tall T waves in hæmopericardium of any ætiology, ascribing it to hæmolysis and local hyperkalæmia168.
The relatively short QT interval may reflect iatrogenous hypercalcæmia provoked by the EMD169.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.