Left Atrial Abnormality & Three Other Blocks


Report:
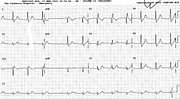
Sinus rhythm 63/min
Left atrial abnormality
First degree AV block
PR 0.36”
Left anterior hemiblock
Right bundle branch block
LVH voltage
RaVL 14 mm
Comment:
The P wave is 0.16” (4 mm) long in lead 2 and, like the classical P mitrale of old, it disports a prominent notch. The notch has an inter-peak distance of more than 1 mm, making the notching electrocardiographically significant. In V1, there is the expected increase in the PTF, the negative part of its P wave exceeding 1 x 1 mm. Full hand.
The more euphonious P mitrale was replaced (by pedants) with LAA because the mitral valve is now rarely responsible for the above appearances and an interatrial conduction defect – in Bachman’s bundle – seems to be the mechanism of the ECG changes. The underlying conditions include left atrial dilatation, hypertrophy, hypertension and, rarely, right atrial enlargement.
The trace could be called trifascicular block, implying the 1o block to be due to intraventricular conduction problems. This is usually not so, as this patient demonstrates with Wenckebach AV block and really long AV conduction times on another occasion (27a).
Fig 27b is another example, with typical LAA in lead 1. There is no obvious PTF deflection in V1, but what looks like PR segment is depressed: that’s where the PTF is spent. Most of the borderline-long PR interval in the limb leads is occupied by P wave itself, invoking Macruz index against the diagnosis of 1o AV block36.
Terminal negativity in Lead 3 is “one of the best signs”37 of LAA. It is, as Schamroth points out, “usually neglected in clinical cardiology”, as bifid P in Lead 1 and marked PTF in V1 tend to steal the show. In the original ECG, the terminal negativity in Lead 3 is barely visible , the late P wave being isoelectric. It may be one the best signs of LAA, but it is not always there.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.