Electromechanical Association


Report:
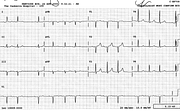
Probable multifocal atrial tachycardia (MAT) 122/min
Vertical heart position
Nonspecific T wave changes
Movement artefact V2-3
Comment:
The earliest ECG sign of emphysema is the shift of P wave axis in the limb leads to beyond +70o. This is of course valid only for sinus P waves, as seen in the traces below. Sometimes it is the only sign. In this trace, the only one is the vertical position (aVL and aVF converging), unusual for the patient’s age – that’s why it’s reported. The MAT is itself a marker of respiratory failure. Relatively narrow QRS complex (less than 0.08” here) is also characteristic of emphysema, but this remains to be validated.
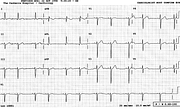
A trace taken six days previously (Fig 193a) shows convincing P pulmonale. The different appearance may reflect more marked pulmonary hypertension or different atrial conduction at the time.
The interesting thing is the presystolic and systolic wriggle in the anteroseptal leads. I went to see the patient and, sure enough, there was a prominent pulsation at the left sternal edge (and the epigastrium – maybe that’s where the impulses were originating).
My impression is – again, unvalidated – that digitalised ECG systems produce jerkier, less well filtered traces than the old stylus machines writing directly on paper rolls. In this case, the artefact could be of some clinical value: a potential project for an ambitious Cardiology Registrar. True, the LSE artefact was not present in the trace with the big P pulmonale – but the chest was probably more expanded then – or else the lead - or the patient - were positioned differently!
Yet another trace, also in sinus rhythm, is shown in Fig 293b, with more modest RAA. The precordial impulse is still there. Weaning “chronic lungers” is often quite protracted; their arrival to ICU makes everyone sigh.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.