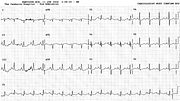
Sinus Tachycardia in Mitral Stenosis

Report:
Sinus tachycardia 114/min
Left atrial abnormality
Comment:
The trace is not really suggestive of mitral stenosis. Apart from the obviously increased PTF in V1, the only clue – a weak one - is small R wave in L1.
Yet he was one of the most interesting cases of MS I treated in ICU. He had severe pulmonary œdema in Casualty and had to be intubated; an echocardiogram showed some “mitral valve thickening”. A Cardiologist missed the physical signs (as did many others) and misread the echocardiogram; he had to be persuaded to come to ICU and repeat the echo, still claiming the initial one was of “good quality”. It was: I merely wanted him to save face. A tact of a Versailles diplomat is required in these situations.
But the real interest lies elsewhere. He could not be extubated: attempts at weaning lead to marked tachycardia (Fig 47a) and oedema welling up the tube. I gave him frequent boluses and eventually an infusion of metoprolol and extubated him in an hour, without diuretics. Something one dreams of doing but rarely has the opportunity.
The patient underwent a mitral valve replacement a few months later.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.