Pædiatric Right Ventricular Hypertrophy
Report:
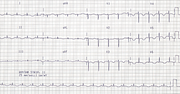
Probable flutter 300/min with 2:1 block
Right axis deviation
Right ventricular hypertrophy
Comment:
In children with congenital heart disease the abnormal RAD is usually manifest as S1S2S3 morphology. The qR in V1 indicates that it is a true RAD, due to RVH.
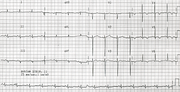
In L2 there is a what looks like a rather squat, rounded secondary R wave. It is almost certainly a second F wave, falling exactly in-between the easily seen atrial deflections. The proof, as often happens, is in a repeat trace, with variable block (Fig 56a below).
The next two tracings (Figs 56b, 56c) show junctional and sinus rhythms, post-cardioversion. The former has retrograde conduction.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.