ST Segment Depression in Pericarditis

Report:
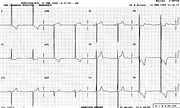
Sinus rhythm 84/min
Borderline left atrial abnormality
Left ventricular hypertrophy voltage
ST segment elevation c/c pericarditis
Comment:
Even with a somewhat wobbly baseline, there is ST depression in V1. This is not a true reciprocal change: it is isolated and the rest of the trace is typical of acute pericarditis. This is quite common in pericarditis, a feature of rS complexes in the frontal leads, too, when present. Sometimes, like in Case 35, such leads merely do not participate in ST elevation.
The proof that the repolarisation changes are due to pericarditis (in reality, epicarditis, since pericardium is electrically silent) is the trace taken two days later, virtually unchanged (Fig 60a).
The LVH voltage with its associated LAA indicates that other, older cardiac pathology may exist here. I looked up the patient’s records: he had mitral valve prolapse with incompetence severe enough to cause pulmonary hypertension, and was booked for MVR. The LVH here is of the volume overload type, with T waves still upright (they may have been large once). Another feature of mitral incompetence LVH (from somewhere in Schamroth) is relatively small S wave in V1.
Thus it came as no surprise when, a few days later, he developed AF (Fig 60b). Pericarditis per se does not cause atrial arrhythmias47.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.