Single Failure to Capture

Report:
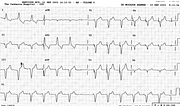
Sinus rhythm 63/min 2
Complete AV dissociation 4
Pacemaker rhythm 80/min 2
Single failure to pace 4
Comment:
AV block cannot be accurately diagnosed here: the atrial (sinus) rate is too slow and the ventricular (pacemaker) rate too fast. Just before the pacemaker insertion, the patient was in 2:1 AV block (Fig 104a) with the ventricular rate 34/min and the atrial 68/min. Alternate P waves there were blocked even further from the preceding QRS complex than the blocked P wave seen preceding the pause created by the temporary failure to pace.
That P wave resembles, superficially, a blocked atrial ectopic, the well-known Marriott’s commonest cause of a pause. It is the reason for including this trace in this collection: so many have misdiagnosed it!
The paced complexes show typical QS morphology in the inferior and all the precordial leads.
An AV block in the setting of inferior infarction would be expected to resolve within days. The only action required here would be to continue monitoring or, perhaps, increase the temporaryunit’s output.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.