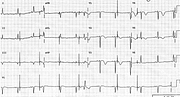
Atrial Pacemaker: Intermittent Failure to Sense

Report: Adler Roy 18/4/99 11065929
Sinus rhythm 66/min 1
Atrial pacemaker discharge 53/min
Intermittent failure to sense 2
Pacemaker capture beats 2
Phasic aberrant RBBB conduction 2
Left atrial abnormality (LAA) 1
Anterior infarction, indeterminate age 2
Nonspecific ST/T changes 0
Comment:
The large atrial pacing spikes disappear in the middle and at the end of the recording, indicating that the failure to sense is only intermittent. There is no problem with atrial pacing: the atria are captured whenever the spike is far away enough from the preceding P wave to find them non-refractory. The apparent R-on-T pacing is no problem here – the pacing electrode is in the atrium while the T waves are, of course, ventricular2.
There are three early beats rewarding the persistent pacemaker with atrial capture. The second one has RBBB morphology. It is a QR rather than RSR’ complex in V1 since its primary R wave is amputated by the previous anterior infarction also responsible for the QS complexes preceding and following it. The reason for its aberrancy is that it is the earliest – most premature – of the three capture beats and the ratio of its cycle length and the preceding cycle’s is smallest. The long-short sequence, rather than the absolute rate, is responsible for the aberrancy, since the refractory period of the bundle branches (and everything else) is directly proportional to the length of the preceding cycle. That’s why Schamroth distinguishes it as phasic rather than rate-dependent aberrancy3. The cycle length discrepancy is much less for the other two capture beats.
Is there any merit in reporting the nonspecific ST/T changes as well as myocardial infarction of uncertain age? There is in this case. Although the repolarisation abnormalities may represent the fait accompli of an established infarction, it would be impossible to exclude current ischaemia or other causes of T wave inversion. The most interesting (to me, at least) of those other causes would be previous ventricular pacing or LBBB conduction4.
The evidence for anterior infarction comprises more than QS in V1 and poor R wave progression: there is no “septal” q wave in V6, either. The distinction from incomplete LBBB (also an R complex in V6) is that the voltage of the latter is almost always large.
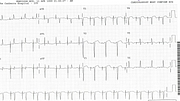
Below (Fig 2a) is the faster pacing rate required in the immediate postoperative period; it is usually set at 90/min. Post-infarct ECG with RBBB and LAHB throughout is shown in Fig 2b.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.