Unusual Mechanism of Escape-Capture Bigeminy
Report:
Sinus rhythm 0.5
SVEBs, blocked, in (atrial) trigeminy 2
AV sequential pacemaker, atrial-sensing (probably DDD) 0.5
Failure to sense SVEBs 4
Atrial-paced escape beats 0.5
Ventricular bigeminy (atrial trigeminy!) 2
Nonspecific T wave changes 0.5
Comment:
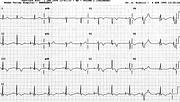
The blocked SVEBs occur only after sinus P waves, with a relatively fixed coupling interval. They look only slightly different from sinus P waves; otherwise they could be blocked sinus P waves themselves. Obviously, the pacemaker agrees in thinking they look different and ignores them, terminating the long pauses with its own atrial-paced P waves. Perhaps its upper rate limit is set quite low (about 94/min) or the PVARP is very long and it chooses to ignore them, but this is unlikely.
The pacing AV interval is set at 0.20”, just slightly longer than the patient’s native PR interval of 0.19”. The fifth QRS complex appears to be preceded by a P wave without a pacing spike, due to respiratory swing of the spikes; its spike is visible in aVL above. The paced P waves also look similar to sinus P waves, indicating a high-atrial position of the electrode tip.
The last capture beat in the rhythm strip is made up of a sinus P wave and a paced ventricular complex: the native PR interval has lengthened slightly and the ventricle became activated by the ventricular lead of the pacemaker, programmed to fire 0.20” after the P wave (sinus or atrial-paced)26. This is the only ventricular-paced complex here. It looks narrow, suggesting ventricular fusion between the sinus and the pacemaker impulses, but this is not so: above it, simultaneous leads V4-6 show it to be quite plump at 0.16”. It only looks narrow in Lead 2 because of its initial isoelectric segment. A blocked SVEB causes a late bump on the descent of its T wave, continuing the atrial trigeminy.
Most of the other QRS complexes, both of sinus and atrial-pacemaker origin, are also preceded by ventricular pacemaker spikes. The spikes coincide with the QRS onset but do not contribute to the ventricular complex. One can tell: the two QRSs not preceded by a spike look exactly the same – no fusion in any of them! The beats with (non-contributory) spikes are called pseudofusion beats.
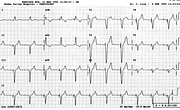
Below, the patient is in sinus rhythm throughout, with atrial-sensing ventricular pacing throughout. Her own PR interval lengthened (or AV conduction failed altogether) and the pacemaker, after waiting 0.20” for something to happen, chipped in. Its beats have the expected LBBB/LAD look.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.