2:1 & Advanced 2o AV Block
Report:
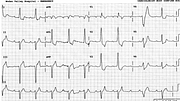
Sinus tachycardia 125/min
Left atrial abnormality (LAA)
Second degree AV block, 2:1 & advanced
First degree AV block (PR 0.28”) in conducted beats
VEB (ventricular escape beat)
Left anterior hemiblock
Right bundle branch block, atypical
Left ventricular hypertrophy with ST/T changes
Comment:
The broad S wave in V1 makes one consider superimposition of a P-terminal force of a P wave, but this is not the case: the real P waves are in their expected positions. The complex looks bizarre in all the right precordial leads, suggesting more than a pure conduction system disease. This is confirmed by the ST/T changes in Lead 1 and aVL, or V4-5.
A 2o AV block is advanced if there is less than 50% conduction of the supraventricular impulses occurring at a reasonable rate. This patient’s rate is reasonable (defined as what one thinks is reasonable!) but, even here, a slower rate may result in 1:1 conduction. There is only one instance of advanced block here, with two consecutive blocked P waves. There may have been more, but the escape beat prevents the potential conduction ratio from being revealed. We are not to know whether the P wave following the two nonconducted ones would have been conducted, were it not for the VEB.
I am not sure whether 2:1 block should be called advanced. Marriott opposes this69 and this is good enough for me. There is certainly nothing wrong calling the 2:1 block what it actually is: 2:1 block!
The QRS has lost its septal r and terminal S wave in lead 1 and looks like LBBB rather than RBBB: it’s on the way to becoming standard masquerading BBB when aVL loses its q wave too.
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.