VEBs & U Waves: Hypokalæmia
Report
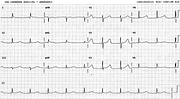
Sinus rhythm.
Sinus arrhythmia.
VEBs, bigeminy.
Prominent U waves consistent with hypokalæmia.
Comment:
The ECG monitor alarmed at the heart rate 34/min. This need not be merely spurious bradycardia, a mistake in the first place, due to negative VEB polarity: the pulse produced by the VEBs may be unrecordable as well.
"Renal" patients not infrequently become hypokalæmic due to the (not entirely unfounded) belief that potassium supplementation may be hazardous. This patient's ectopic activity disappeared with 10 mEq/hour of KCL over 2 hours; the serum potassium rose from 3.1 to 3.9 mEq/L. ICU interventions to suppress ventricular ectopic activity as a rule remain confined to correcting electrolytes, hypoxæmia, pH and the hæmodynamics; they are less frequent but more successful than those relying on antiarrhythmic drugs elsewhere.
In the top strip one can map out the nadir of the P waves throughout. It produces a negative notch in the ST segment of the VEBs.
The single VEB in the bottom trace follows the longest sinus cycle, illustrating the tendency of VEBs to follow long cycles. That may be why bigeminy begets bigeminy – the rule of bigeminy. It does not always hold: this VEB (probably) failed to evoke another in its wake.
Speaking of elsewhere, below is a strip from CCU (Fig 268a). Shallow inverted T wave merging into an upright U wave. Here the appearance was due to combination of digoxin and quinidine. The potassium, checked prior to cardioversion, was normal (4.2 mEq/L). There is no substitute for measuring the potassium level.
Hypokalæmia mimicry by digoxin - quinidine combination was stressed by Marriott201. Quinidine is becoming a rarely used drug nowadays; the strip may not survive more than a few more years in this Library.
Collections
Tags
vebs bigeminal u wave hypokalæmia digoxin spurious hypokalæmia with quinidine marriott
If you have any suggestions for or feedback on this report, please let us know.

Hi, can we chat about some terms and conditions?
The library and it's records are licensed under the Creative Commons Attribution 4.0 International license.
You are free to:
- Share — copy and redistribute the material in any medium or format for any purpose, even commercially.
- Adapt — remix, transform, and build upon the material for any purpose, even commercially.
- The licensor cannot revoke these freedoms as long as you follow the license terms.
Under the following terms:
- Attribution — You must give appropriate credit , provide a link to the license, and indicate if changes were made . You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits.
By clicking agree below, you are agreeing to adhere to CC BY 4.0.